Sparber-Sauer M, Ferrari A, Spunt SL, Vokuhl C, Casey D, Lautz TB, Meyer WH, Walterhouse DO, Pajtler KW, Alaggio R, Schmidt A, Safwat A, Timmermann B, Dall'Igna P, Chen S, Weiss AR, Orbach D.
Pediatr Blood Cancer 2023 Feb;70(2):e30116. doi: 10.1002/pbc.30116. Epub 2022 Nov 28, 2023 Feb 6. doi: 10.1002/cam4.5671. Online ahead of print.
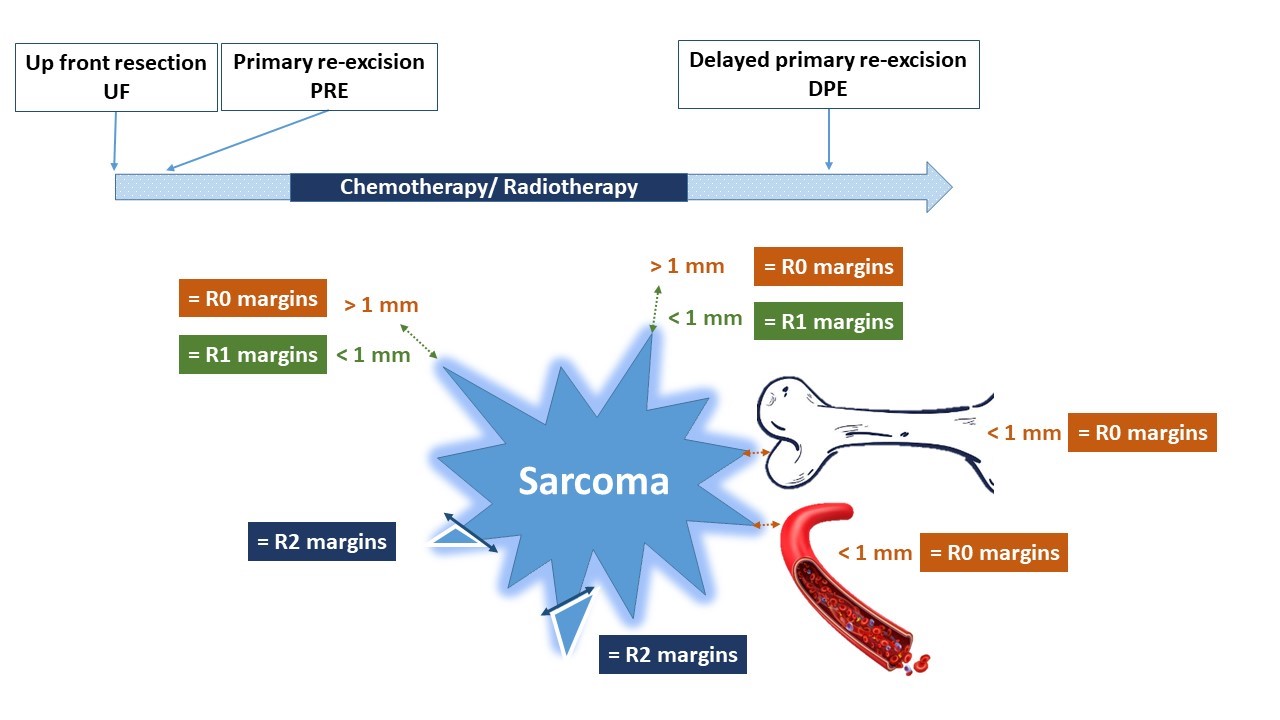
Margin status following surgery in children, adolescents and young adults with soft tissue sarcomas is controversial and has been defined differently by various specialties, with definitions changing over time and by cooperative group. The International Soft Tissue Sarcoma Consortium (INSTRuCT) is a collaboration of the Children’s Oncology Group (COG) Soft Tissue Sarcoma Committee, European pediatric Soft Tissue sarcoma Study Group (EpSSG), and the European Cooperative Weichteilsarkom Studiengruppe (CWS) devoted to improving patient outcomes by pooling and mining cooperative group clinical trial data. The INSTRuCT non-rhabdomyosarcoma soft tissue sarcoma (NRSTS) working group aimed to develop international harmonized recommendations regarding surgical margin assessment and definitions in children and adolescents with soft tissue tumors. This review addresses accepted principles and areas of controversy, including the perspectives of surgeons, pathologists, radiation oncologists, and pediatric oncologists, to develop a framework for building common guidelines for future research. To answer unresolved questions and address major deficiencies in the existing systems for margin classification, the authors propose a new margin classification system. This new system includes information on PRE and the difference between “unresected tumor” which potentially can be resected by re-excision and “unresectable tumor”. Furthermore, the depth/width of the margins must be documented precisely in the pathology report, and should include areas of tumor necrosis at the margin as well as margins adjacent to specific anatomic boundaries. Moreover, information on the margin status for primary delayed resection that were achieved post-chemotherapy, post-RT or both must be detailed. The tumor grade and innate tumor biology highlight the heterogeneity of NRSTS and these data should be collected by registries and analyzed in future trials to further inform prognostic value and treatment methods. Although the authors acknowledge that some important data are lacking to optimally define “margins” in pediatric NRSTS, we have proposed consensus definitions to serve as a tool for future prospective studies.